Why Sleep Alone Doesn’t Fix It
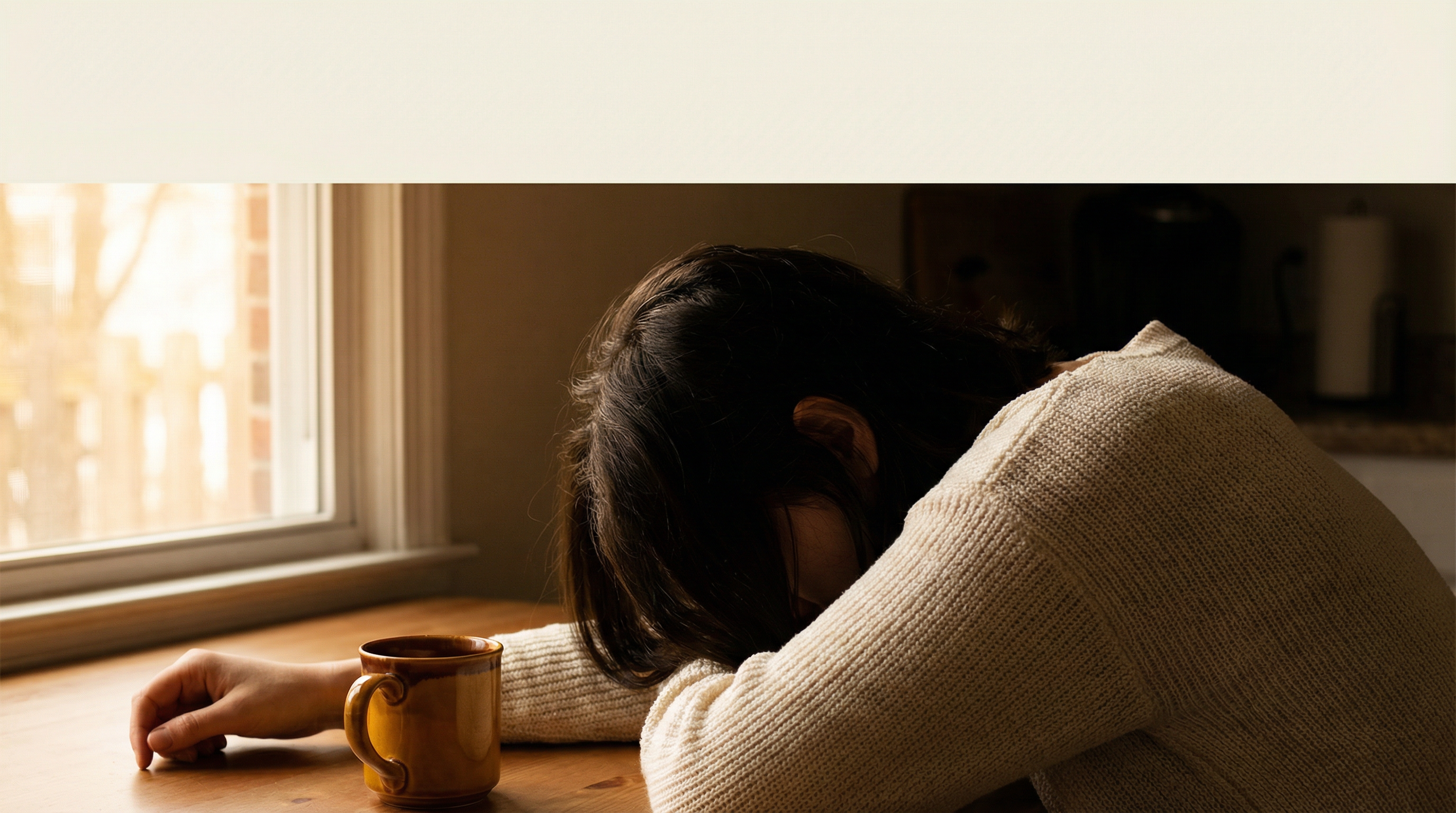
The conventional explanation for maternal exhaustion is sleep deprivation. And sleep deprivation is real, significant, and contributes enormously to how mothers feel. But many mothers — even those whose children have grown past the infant stage, even those getting seven or eight hours of sleep most nights — still experience a level of tiredness that sleep doesn’t seem to fix. Something else is happening.
That something else is hypervigilance: the brain’s persistent threat-monitoring state, which in mothers operates at a level that most people outside caregiving never experience. Understanding hypervigilance is the key to understanding the exhaustion that sleep cannot resolve.
Is a Foggy Brain Holding You Back?
Download the free Brain Fog Fix Guide and discover the 12-minute audio technique that thousands use to restore mental clarity — no supplements, no meditation required.
Get the Free Guide →What Hypervigilance Is and Why Mothers Have It
Hypervigilance is the nervous system’s response to an environment perceived as requiring constant monitoring for threats. In clinical contexts, it is associated with post-traumatic stress disorder. But a subtler, functional form of hypervigilance is a normal feature of motherhood — one that evolved over hundreds of thousands of years precisely because it served the survival of vulnerable offspring.
The maternal brain is structurally primed for heightened threat detection. Research from the Journal of Child Psychology and Psychiatry and other sources has documented that new mothers show enhanced amygdala reactivity to infant stimuli — their brains respond more intensely to cues of infant distress than non-mothers do. This is adaptive: it ensures that a baby’s cry is processed as urgent, that a child’s silence in the next room is noticed, that a change in breathing pattern registers as a potential concern.
But the amygdala does not distinguish between a genuine threat and the ambient low-level risk-monitoring that motherhood requires. The same neural pathway that scans for genuine danger also processes:
- The awareness that a child hasn’t come home from school yet
- The monitoring of a toddler near a swimming pool
- The tracking of a teenager’s location and emotional state
- The anticipatory anxiety about whether a child is eating enough, developing normally, being bullied
- The half-listening for sounds from upstairs even during the one hour you had to yourself
All of these require the amygdala to remain partially activated. And a partially activated amygdala means a partially activated stress response — elevated cortisol, maintained sympathetic tone, suppressed parasympathetic recovery. Not quite fight-or-flight, but nowhere near genuine rest.
The Brainwave Cost of Constant Scanning
Neurologically, hypervigilance keeps the brain operating in a high-beta frequency range (approximately 15–30 Hz) — the electrical oscillation pattern associated with active alertness, anxiety, and vigilant problem-solving. This is the appropriate state for responding to demands. It is a deeply inappropriate state for recovery.
Recovery — genuine neurological recovery — requires the brain to shift into lower frequency states: alpha (8–12 Hz, relaxed awareness), theta (4–8 Hz, deep relaxation, memory consolidation), and delta (0.5–4 Hz, deep sleep). These are the states in which the brain repairs the damage done by stress hormones, consolidates memories from the day, restores neurotransmitter levels, and processes emotional experience.
A brain maintained in hypervigilant high-beta state through a combination of neurobiological priming and genuine environmental demands struggles to enter these recovery frequencies even when the external pressure is temporarily absent. This is why many mothers describe lying in bed, exhausted, and still being unable to “turn off” — the brain has been in high-beta mode so consistently that transitioning to alpha or theta requires a deliberate intervention rather than happening naturally.
Our complete brainwave science guide covers the different frequency states and why transitioning between them matters so much for recovery and performance.
Cortisol Accumulation: The Compound Interest of Stress
Every activation of the stress response produces a cortisol pulse. Under normal conditions, cortisol rises in the morning (the cortisol awakening response), performs its activating function, and falls back to baseline by evening. This pattern is called the diurnal cortisol curve, and it is associated with good health, energy, and cognitive function.
In mothers managing chronic hypervigilance, this curve flattens. Cortisol is elevated throughout the day — never peaking dramatically, never dropping to baseline. This “flat” cortisol pattern is associated with chronic fatigue, impaired immune function, reduced cognitive performance, and heightened emotional reactivity. It is the neurochemical signature of the mother who is “always tired” in a way that does not respond to rest.
Chronic cortisol elevation also affects the brain directly, as described in detail in our article on brain fog and stress: it reduces hippocampal volume (impairing memory), suppresses prefrontal cortex activity (impairing decision-making and emotional regulation), and sensitises the amygdala (making threat responses more intense and more easily triggered). Each of these effects makes the experience of motherhood harder, which in turn generates more stress, which perpetuates the cortisol pattern. It is a loop that effort and willpower cannot break from the inside.
The Mental Load as Neurological Burden
Separate from the emotional hypervigilance, there is the cognitive hypervigilance of the mental load — the invisible labour of tracking, planning, and coordinating everything that keeps a family functioning. Research has consistently shown that this labour falls disproportionately on mothers in heterosexual partnerships, independent of employment status.
The mental load does not live in the background passively. It occupies working memory, requires regular executive function attention to maintain and update, and generates low-level anxiety when any element is at risk of dropping. The mother who is simultaneously listening to a podcast, driving, and mentally reviewing whether she remembered to book the dentist and whether the permission slip was signed is not multitasking — she is serially task-switching, and each switch has a cognitive cost.
Decision fatigue from this constant cognitive demand compounds the hypervigilance-driven physical fatigue into the complete exhaustion that so many mothers experience by evening: emotionally depleted, cognitively drained, and still physiologically activated enough that genuine rest does not come easily.
The Off-Switch: What Actually Works
If hypervigilance is the mechanism, the treatment is anything that reliably activates the parasympathetic nervous system and shifts the brain out of high-beta state. The challenge for mothers is that most effective parasympathetic activators require a condition that is itself difficult to achieve: the absence of the trigger. You cannot genuinely down-regulate the amygdala’s threat-scanning while you are still in the environment that the amygdala is monitoring.
This is why short, discrete, complete separations from the caregiving environment produce disproportionate recovery benefit. The brain needs a clear signal that the monitoring can pause. Even 12 minutes in a different room with headphones on — creating physical and perceptual separation from the triggers — gives the amygdala the input it needs to begin deactivating.
Theta brainwave audio is particularly effective in this context because it provides an active neurological intervention rather than relying on passive relaxation. The brain’s frequency-following response means that theta audio actively pulls neural oscillations away from the high-beta hypervigilant range toward the theta restorative range. This is not just psychological relaxation — it is a measurable shift in the brain’s electrical state.
Try The Genius Song risk-free — $39 one-time, 90-day money-back guarantee. The 12-minute format is specifically calibrated for the time windows that caregivers actually have.
For practical self-care options that fit within real caregiver schedules, including theta audio and four other evidence-backed interventions, see our guide to self-care that takes 12 minutes or less.
Why This Validation Matters
The experience of explaining your exhaustion to someone who does not understand the neurological mechanism of hypervigilance — who says “you should get more sleep” or “you need to relax more” — is profoundly isolating. Because you know it is not simply about sleep. You know it is not simply about relaxing. Your body knows the difference between genuine rest and the pale imitation of rest that hypervigilance permits.
The neuroscience confirms what your body is telling you: this is a real physiological state with measurable neurological correlates. It is not a personality problem, a motivation problem, or a failure of effort. It is a brain running a programme that evolution designed for a very different caregiving context — one in which genuine rest was available between periods of active vigilance, in which the community around a mother shared the monitoring burden, and in which the cognitive demands of managing a complex modern life did not compound the already-significant demands of keeping children safe.
You are not weak. You are exhausted under genuinely exhausting conditions. And the way through is not more effort — it is smarter recovery. The full framework for that recovery is in our caregiver brain fatigue guide.